A Guide to the Oesophagus.
We’d wager that if ‘organs you’d find in your chest’ was a category in Family Fortunes, the oesophagus wouldn’t even make the top five. It’s a structure you probably don’t give much thought to in your day-to-day life – you might think it’s just a tube that doesn’t really do much except act as a passageway to get your food to your stomach, but it’s actually a really sophisticated piece of your anatomy that is controlled both voluntarily and involuntarily.
Want to learn more about it? Let’s dive in.
The oesophagus is a fibromuscular tube (about 25cm in length in adults) that connects your throat to your stomach. Everything you eat or drink passes down your oesophagus, while the air that we breathe travels down the trachea (windpipe), which sits in front of the oesophagus, to our lungs.
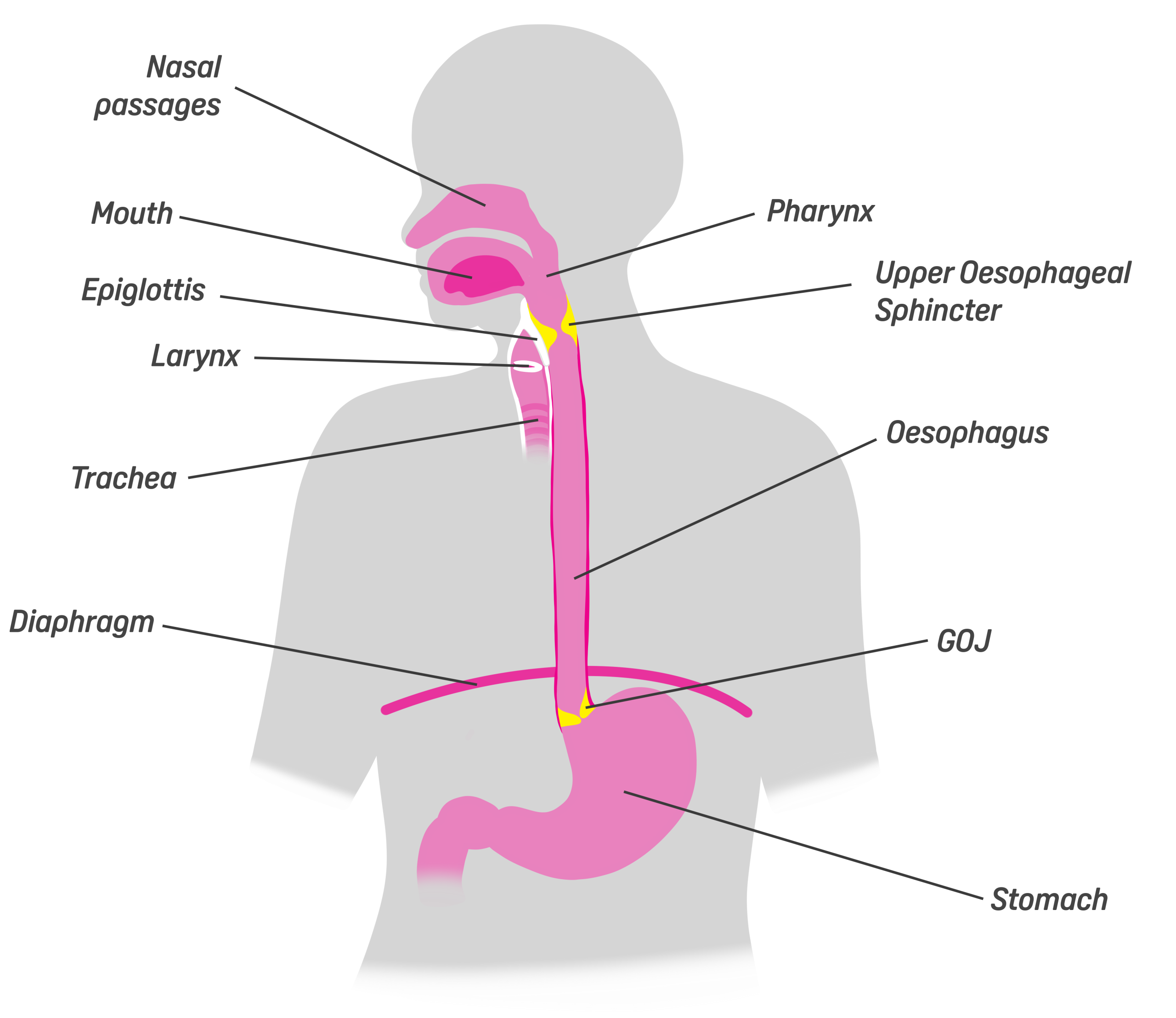
While the trachea is supported by C-shaped rings of cartilage to keep it open, the oesophagus is a highly muscular structure that contracts to push food down into the stomach. It starts with a voluntary action – swallowing – but as soon as your food reaches the pharynx, the rest is done automatically by way of peristalsis. These involuntary, wave-life contractions push food, drink and saliva down into your stomach. The segment behind the bolus (the stuff you’re swallowing) contracts, while the segment ahead relaxes – this pattern continues down the oesophagus until the bolus reaches the gastro-oesophageal junction (GOJ) – the gateway to the stomach. This means food can still travel down your oesophagus if you’re lying down – although we love a cheeky bedtime snack, it is best not to eat lying down due to the higher risk of choking.
At each end of the oesophagus is a sphincter that prevents food from travelling back up the wrong way, although these open when we are unlucky enough to vomit. The lower sphincter that sits at the bottom of the oesophagus is referred to as the GOJ or sometimes as the EGJ or LOS – when we experience acid reflux, it can be an indication that the GOJ isn’t quite doing its job properly.
Tissues in the oesophagus...
To understand how the oesophagus works – and how disease affects it – you have to understand its layers and the different cell types. We’ve popped a glossary at the bottom of this page so if you’re unfamiliar with any of the terms in this article, you can find their meanings there.
The innermost layer, the mucosa, is composed of three parts: epithelium, lamina propria, and muscularis mucosae.
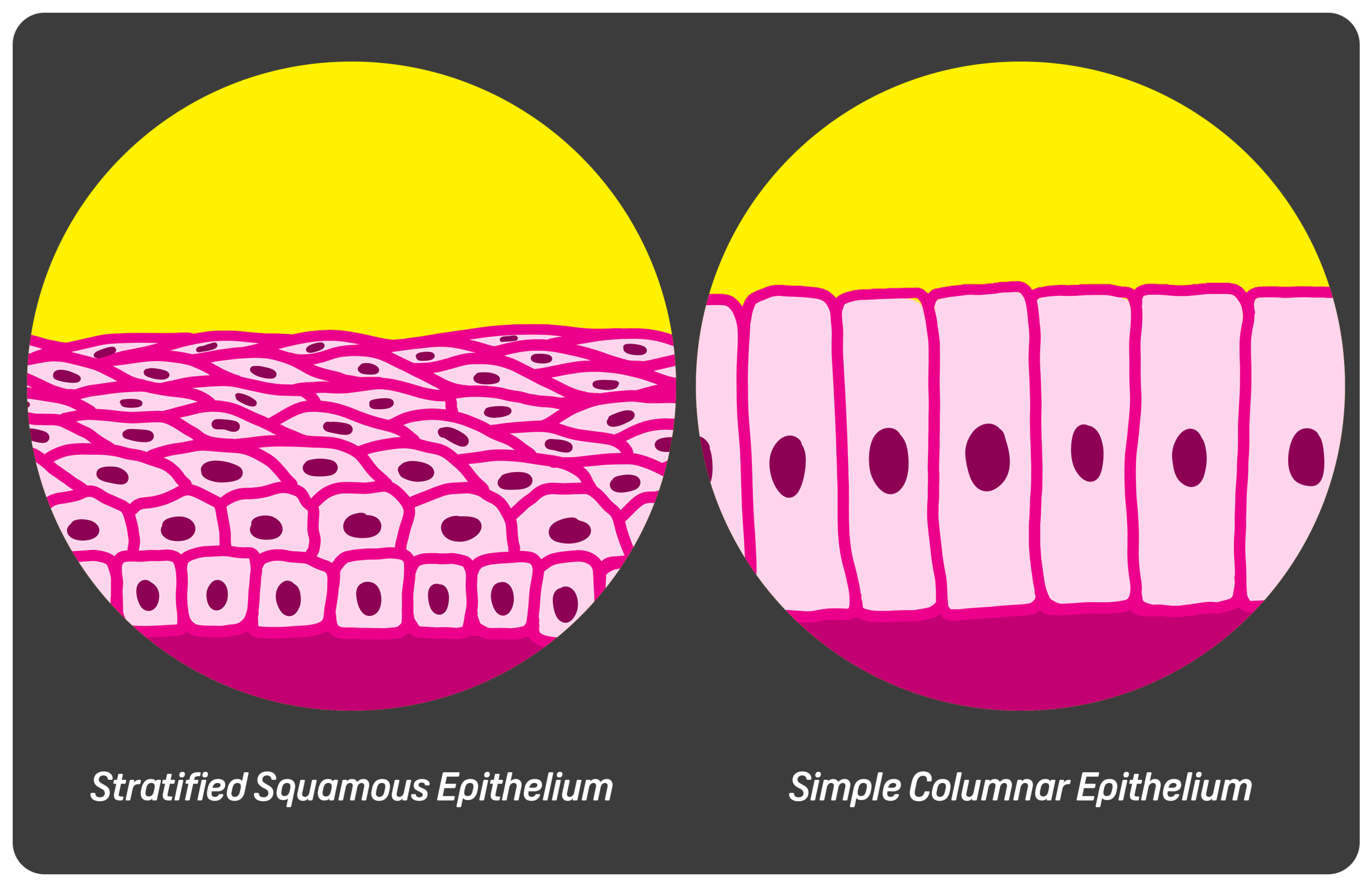

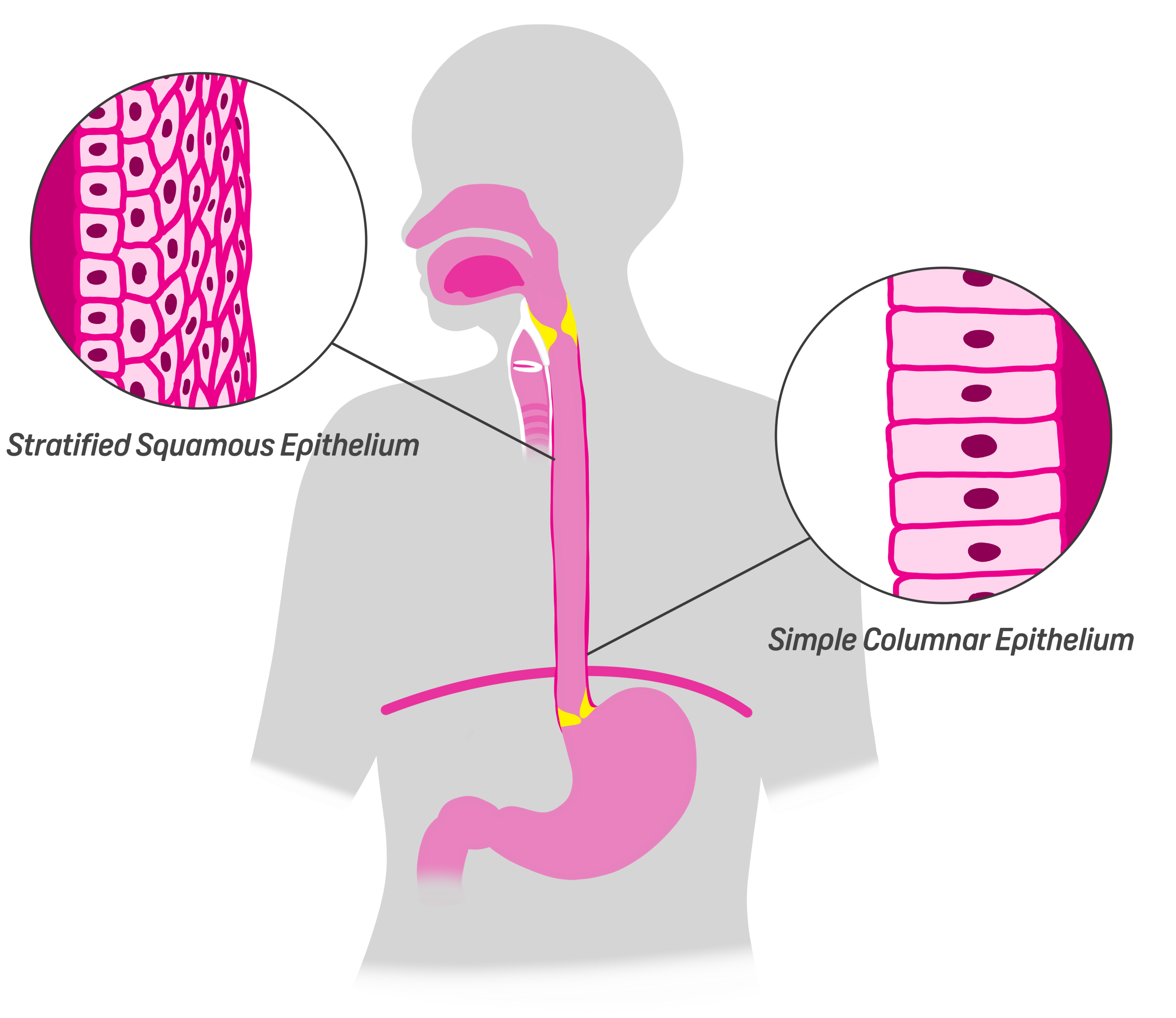
The epithelium lining most of the oesophagus (especially in the higher portions) is something called stratified squamous epithelium. These are flat, layered cells arranged like protective tiles. Their primary function is mechanical protection – every time you swallow something rough (a crust of bread or a crisp, for instance) these cells absorb the abrasion. They are not designed to secrete, digest, or absorb nutrients – their job is durability. They can do this because they continuously renew themselves. Basal stem cells located in the deeper layers divide and migrate upward, replacing cells shed at the surface. This regenerative capacity is essential because the oesophagus experiences constant friction – so next time you enjoy something particularly crunchy, give a mental high-five to these cells.
Further down the oesophagus near the GOJ, we have columnar cells. These cells don’t regenerate as quickly as the stratified squamous cells higher up because their purpose is not to endure mechanical stress. These cells are tall and rectangular and their purpose is to both secrete mucus for lubrication and for chemical resilience due to its close proximity to the stomach. In certain pathological states (such as Barrett’s Oesophagus), the squamous epithelium is replaced by metaplastic columnar epithelium. This change increases acid resistance but also raises cancer risk.
Beneath the epithelium lies the lamina propria, a connective tissue layer containing blood vessels, immune cells, and structural support. Immune surveillance happens here; lymphocytes and other immune cells are constantly on the lookout for pathogens or injury in the oesophagus.
At the base of the mucosa lies the muscularis mucosae; a thin layer of smooth muscle. Its subtle contractions help maintain mucosal tone and assist in clearing residual material.
Beneath the mucosa lies the submucosa, a thicker connective tissue layer containing blood vessels, lymphatics, nerves, and glands. The oesophageal glands located here produce mucus, and that mucus is critical. It lubricates swallowed material, reduces friction, and protects the epithelium from mechanical stress. Without adequate lubrication, swallowing would feel harsh and uncomfortable. The submucosa also houses nerve networks, including components of the enteric nervous system. These intrinsic nerves coordinate local reflexes and contribute to the control of peristalsis.
The next layer down is the muscularis propria; the engine that drives movement. It consists of two layers: an inner circular layer and an outer longitudinal layer. In the upper third of the oesophagus, the muscle is skeletal (striated) muscle. This allows rapid, voluntary initiation of swallowing. In the lower third, the muscle is smooth muscle, operating entirely under involuntary control. The middle third contains a transition zone with a mix of both. The circular layer constricts behind the bolus, while the longitudinal layer shortens the oesophagus segmentally, helping propel contents downward. Together, they create the peristaltic waves.
Embedded between these muscle layers is the myenteric (Auerbach’s) plexus; a network of neurons that coordinates contraction and relaxation. If this neural network malfunctions, motility disorders arise.

The GOJ
At the lower end of the oesophagus lies the GOJ, where squamous epithelium meets the stomach’s columnar epithelium. On endoscopy, this transition is visible as the “Z-line.”
Functionally, the GOJ includes the lower oesophageal sphincter (LOS), a specialised region of smooth muscle that maintains a resting tone. This tone keeps the junction closed, preventing acidic stomach contents from refluxing upward. When a bolus approaches, the LOS relaxes momentarily to allow passage of food, then contracts again.
The diaphragm contributes to this barrier; as the oesophagus passes through the diaphragm, the surrounding muscle fibres change the sphincter pressure. The angle at which the oesophagus meets the stomach (the angle of His) also helps create a mechanical anti-reflux effect. When this coordinated barrier weakens, acid reflux occurs.

How to take care of your oesophagus
Looking after your oesophagus starts with one core principle: minimise irritation and keep acid reflux under control. Ongoing exposure to stomach acid is one of the biggest threats to oesophageal health, so reducing reflux is essential. Practical steps include maintaining a healthy body weight, avoiding large or late evening meals, and limiting foods and drinks that trigger symptoms - such as alcohol, caffeine, and high-fat or acidic options. It also helps to remain upright after eating rather than lying down straight away.
Smoking is particularly harmful to the oesophagus. It relaxes the lower oesophageal sphincter - the valve that keeps stomach acid where it belongs - and significantly increases the risk of cancer. Quitting smoking is one of the most important protective measures you can take.
Repeated vomiting, persistent acid reflux, and untreated inflammation may eventually lead to scarring or abnormal cellular changes in the lining of the oesophagus. Direct damage is another concern. Swallowing corrosive substances, taking medication without sufficient water, or regularly consuming very hot drinks can all injure the delicate tissue.
Simple daily habits make a difference: eat slowly, chew food thoroughly, drink enough fluids, and seek medical advice if you experience ongoing heartburn or difficulty swallowing. Early assessment can prevent more serious complications.
To explore oesophageal conditions in more detail, read our comprehensive guide here
Glossary
Acid Reflux
Stomach acid and contents flowing back up the oesophagus
Angle of His
The angle created by the shape of the anatomy at the entrance to the stomach
Barrett's Oesophagus
(Barrett's Metaplasia, Barrett's Disease) A condition where the lining of the oesophagus changes due to chronic acid damage, usually from a long-tern reflux disorder.
Basal stem cells
Undifferentiated, self-renewing cells at the lowest level of the epithelium that divide to produce new epithelial cells
Bolus
A small mass of substance, i.e. chewed food
Columnar cells
Tall, narrow, pillar-like epithelial cells involved in secretion
Diaphragm
The muscular partition that separates the chest cavity from the abdominal cavity
EGJ
Esophagogastric junction - same as the GOJ
Epithelium
The thin tissue forming the uppermost layer of a body's tissue, including the inner lumen of the oesophagus
Fibromuscular
A structure in the body composed of both fibrous and muscular tissues
Glands
Small organs in the body that secrete substances
GOJ
Gastro-oesophageal junction: the junction between the oesophagus and the stomach
Lamina propria
A layer of loose connective tissue found beneath the epithelium of mucous membranes
LOS
Lower oesophageal sphincter - a ring of smooth muscle that closes and opens between the oesophagus and the stomach
Lumen
The inner, open space within a tubular structure
Lymphatics
The lymphatic system - a network of nodes and vessels that support the immune system
Metaplastic
Abnormal cells
Mucosa
A mucous membrane in the body
Muscularis mucosae
A layer of smooth muscle that forms the outermost layer of the oesophagus
Myenteric plexus
(Auerbach's plexus) A network of nerves responsible for coordinating peristalsis
Oesophagus
The tube that connects your throat to your stomach, allowing for passage of food, drink and saliva
Pathological
Relating to disease
Peristalsis
A series of involuntary wave-like muscle contractions and relaxations of the digestive tract that propel food, fluid and waste through the body
Pharynx
Commonly referred to as the throat, the pharynx is located at the back of the mouth and connects to the oesophagus
Sphincter
A ring of muscle that closes and opens to guard a tube in the body
Squamous
Thin, flat cells arranged like scales
Stratified
Arranged in layers
Submucosa
The layer of connective tissue beneath the mucous membrane
Z-Line
Transition point where the squamous epithelium meets the columnar epithelium in the oesophagus
Resources used to inform this article
This article was created using reference material from ScienceDirect, Cleveland Clinic, the NHS website and NCBI.


